






Navicular syndrome causes chronic forelimb lameness in horses. This degenerative condition affects the navicular bone and associated soft tissues within the hoof. It creates pain in the heel region, often seen in both front feet. Management involves corrective shoeing, medication, and specific exercise to reduce discomfort and slow disease progression.
You have a diagnosis of navicular syndrome. A term that means a chronic, degenerative and often painful condition that presents as forelimb lameness. The pathology is in the podotrochlear apparatus, the navicular bone and its associated soft tissue structures within the hoof capsule, resulting in significant, often bilateral, palmar foot pain. So management is a complex interplay of therapeutic farriery, pharmacological intervention and carefully modulated exercise to reduce pain and slow the progression of the disease.
What is Podotrochleosis (Navicular Syndrome)
The initial signs can be frustratingly subtle. What was once fluid movement becomes hesitant, a shortened stride or a head bob. This is the first, often heart breaking, sign of what veterinarians call podotrochleosis or palmar foot pain. It’s a complex and incompletely understood syndrome that targets the caudal (heel) region of the forefeet. And it’s so much more than a sore foot.
Honestly, the onset is insidious. An almost imperceptible decrease in performance. A shortened stride. An increased tendency to trip. Maybe the horse starts to “point” a forelimb at rest, a classic posture to offload the painful heel. The condition creeps into the horse’s life so gradually that owners can’t pinpoint when it started, only that a low grade lameness has become the new normal.
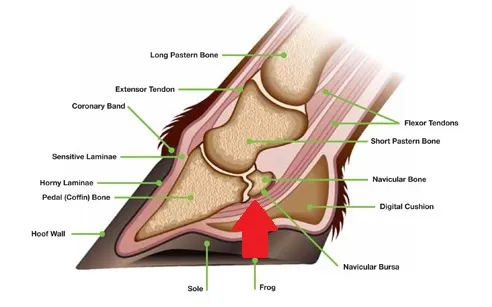
Image source: https://i0.wp.com/springhillequine.com/wp-content/uploads/2018/05/Hoof-breakdown-navicular.jpg?
So what is the pathophysiology? At its core navicular syndrome is a collection of pathologies affecting the podotrochlear apparatus, a critical biomechanical system that includes:
- The Navicular Bone (Distal Sesamoid Bone): A small, shuttle shaped bone behind the distal phalanx (coffin bone). It acts as a fulcrum, redirecting the force of the deep digital flexor tendon.
- The Deep Digital Flexor Tendon (DDFT): A big tendon that runs down the palmar aspect of the limb, glides over the fibrocartilaginous surface of the navicular bone and inserts on the bottom of the coffin bone. Its main function is flexion of the digit.
- Associated Structures: This includes the navicular bursa (a synovial sac that reduces friction between the DDFT and the bone) and the impar and collateral sesamoidean ligaments that stabilise the whole apparatus.
When any of these components are damaged, inflamed or degenerated… that’s where the pain and lameness comes from. It’s a progressive condition. Understanding these mechanics is the first step to effective intervention. Knowledge is power.
Etiology: The Causative Factors and Pathological Cascade
Ever wonder why one horse develops this condition and a herdmate in the same work does not? It’s rarely one insult. The etiology is almost always multifactorial – a complex web of predisposing factors and mechanical stressors that lead to pathology. A full understanding of these factors is essential for a good prognosis.
The primary causative agents are a combination of genetics and biomechanical stress. Consider these main culprits:
- Conformational Deficits: This is key. Poor hoof conformation – a long toe, low heel – increases biomechanical stress on the podotrochlear apparatus. This conformation delays breakover and increases the tensile forces on the DDFT as it articulates with the navicular bone.
- Repetitive Concussive Forces: High impact disciplines like jumping, reining and cutting or consistent work on hard surfaces generates cumulative micro trauma. These shockwaves travel up the hoof and limb and contribute to degenerative changes over time.
- Genetic Predisposition: Certain breeds like Quarter Horses, Thoroughbreds and various Warmbloods have a higher incidence of navicular syndrome, suggesting a heritable component that may influence conformation or tissue resilience.
- Improper Farriery: The farrier is critical. An imbalanced trim or shoeing that doesn’t provide adequate palmar support can introduce aberrant stress patterns that contributes to the onset or exacerbation of the condition.
- Body Mass and Workload: A higher body weight or intense work load increases the force on the hoof structures with every stride.Once these factors are in play, what’s happening at a cellular level? A pathological cascade is initiated. This involves inflammation, ischaemia (reduced blood supply) and degeneration that overwhelms the body’s repair mechanisms. The pain can come from multiple sources:
- Osseous Pathology: The navicular bone itself can degenerate, including the formation of synovial invaginations (often called “cysts”), sclerosis and loss of its smooth fibrocartilaginous surface. This rough surface then abrades the DDFT like a frayed rope over a sharp edge.
- Bursitis: Inflammation of the navicular bursa due to compression and friction is common and very painful.
- Tendinopathy: Lesions or fibre tearing can develop in the DDFT as it’s subjected to increased strain and friction. Significant DDFT damage makes the prognosis very poor.
- Desmitis: Inflammation of the supporting ligaments.
A critical component of this whole process is blood supply. The navicular bone has a precarious blood supply and chronic biomechanical stress can further compromise perfusion. This ischaemia prevents the bone from repairing micro damage, perpetuating a vicious cycle of degeneration, inflammation and further ischaemia. This turns the condition into a chronic, progressive nightmare.
The Diagnostic Process: A Systematic Investigation
So the horse is lame and navicular syndrome is on the list of differentials. The veterinarian’s role now becomes that of a clinical investigator, piecing together the evidence to form a diagnosis.
Initial Clinical Signs
- An intermittent, often bilateral, forelimb lameness that is worse on hard ground or during tight turns (lungeing).
- A shortened, choppy stride often with a “toe-first” landing to avoid painful heel impact.
- Postural “pointing” of one forelimb at rest.
- A general unwillingness to work, including refusals or resistance.
- Increased stumbling.
- Secondary compensatory pain, particularly in the back and gluteal regions, is a common and often-overlooked complication.
The Veterinarian’s Examination & Lameness Exam
A systematic assessment of the horse moving in-hand at a walk and trot, on both hard and soft surfaces, and in circles. Dynamic flexion tests are often used to exacerbate subtle lameness.
- Hoof Tester Application: Precise pressure applied over the frog and heel region can elicit a pain response, helping to localise the discomfort.
- Perineural Anesthesia (Nerve Blocks): This is the diagnostic key. Anesthetic is used to desensitize specific nerves in the heel. If the lameness resolves after a palmar digital nerve block… bingo. The source of pain has been isolated to the caudal third of the hoof.
Diagnostic Imaging: Visualising the Pathology
While blocks confirm where the pain is, advanced imaging is required to determine what is causing it.
- Radiographs (X-rays): The first imaging modality. Radiographs are good for evaluating osseous structures, showing changes like cysts, sclerosis or remodelling of the navicular bone. However—and this is a critical limitation—they provide no information about the soft tissues.
- Ultrasonography: Can be useful for assessing parts of the DDFT and ligaments, but its diagnostic window is limited by the hoof capsule.
- Magnetic Resonance Imaging (MRI): The gold standard. No question. MRI provides a detailed, three-dimensional view of all structures within the hoof, bone, tendon, ligaments and bursa. It gives a complete pathological picture, allowing the most accurate diagnosis and therefore the most informed prognosis. It eliminates the guesswork.
The diagnosis is a synthesis of clinical signs and imaging findings, with the prognosis dependent on the structures damaged and the severity of the pathology.
The Management Protocol: A Multi-faceted Approach
With a diagnosis confirmed, the hard work begins. There is no magic bullet. Management is a long-term, multi-faceted strategy and the owner is central to it. It requires patience, consistency and a team approach with your veterinarian and farrier.
Cornerstone of Care: Therapeutic Farriery
This is the first line of defence. Therapeutic shoeing is a science that alters hoof biomechanics to reduce stress on the podotrochlear apparatus. The objectives are:*
- Easing Breakover: A rolled or rockered toe to make it easier for the hoof to leave the ground, reducing the peak tensile load on the DDFT.
- Providing Palmar Support: Shoes with wider webs, frog-support pads or bar shoes to distribute weight-bearing forces across the whole solar surface and away from the compromised heel.
- Altering the Hoof Pastern Axis: Heel elevation (wedges) can reduce DDFT tension, but this must be managed carefully to avoid other complications.
- Ensuring Mediolateral Balance: Hoof imbalances must be corrected.
- Reducing Concussion: Pads and shock-absorbing materials.
This is not a cure, but it can make the horse more comfortable.
Pharmacological and Biologic Interventions
Farriery addresses the mechanics, medical therapies address the pain and inflammation.
- NSAIDs (Non-Steroidal Anti-Inflammatory Drugs): Phenylbutazone (“Bute”) for acute flare-ups and pain. Long-term use requires careful monitoring due to side effects.
- Intra-bursal/Articular Injections: Corticosteroids into the navicular bursa or coffin joint for potent, if temporary, anti-inflammatory relief.
- Bisphosphonates (e.g., Osphos®, Tildren®): These drugs target bone remodelling by inhibiting osteoclast activity, which can reduce pain associated with osseous pathology. They have been a game-changer for some cases.
- Regenerative Therapies: For cases with significant soft tissue damage, orthobiologics like IRAP, Platelet-Rich Plasma (PRP) or stem cells may be used to promote tissue healing.
The Exercise Paradox: A Fine Line
This is a common point of confusion. Acute pain requires rest, but long-term immobility is bad. The key is subtlety.
During the acute inflammatory phase, stall rest or small-paddock confinement is indicated. But once that phase is controlled, consistent, low-impact exercise is essential. Movement is the main way to promote blood flow in the hoof and adequate blood flow is essential for healing and tissue health. The protocol is turnout and controlled exercise on soft surfaces, with any increase in workload implemented very, very slowly.
The Whole-Horse Approach
Chronic forelimb pain always creates compensatory issues elsewhere. Horses change their gait and posture to protect their painful feet, which puts abnormal stress on their back, neck and hindquarters. This creates secondary pain patterns and muscle soreness. A holistic approach is essential. Adjunctive therapies like chiropractic, massage and core strengthening can make a big difference to the horse’s overall comfort and quality of life.
Emerging Ally: The Role of Red Light Therapy (Photobiomodulation)
Alongside the foundational management pillars of farriery, pharmacology, and controlled exercise, a new generation of non-invasive therapies is gaining traction. Among the most promising is Red Light Therapy (RLT), also known by its scientific name, photobiomodulation (PBM). This therapy uses specific wavelengths of red and near-infrared light to stimulate healing at a cellular level, offering a way to support the body’s natural repair mechanisms without drugs or surgery.

Specific Application for Navicular Syndrome
When you apply these mechanisms to the pathologies of navicular syndrome, the potential benefits become clear. RLT is not a cure, but it can be a powerful adjunctive tool to break the cycle of pain and degeneration.
- Targeting the Ischemic Cycle: The article highlights that a “vicious cycle of degeneration, inflammation and further ischaemia” is what turns this condition into a chronic nightmare. RLT’s ability to improve local blood flow directly counteracts the ischemic component, helping to perfuse the navicular bone and its surrounding structures, thereby promoting an environment conducive to healing rather than degeneration.
- Supporting Soft Tissue Health: For cases involving tendinopathy of the DDFT, bursitis, or desmitis of the supporting ligaments, RLT can be invaluable. The increased cellular energy and reduced inflammation can aid in the repair and remodeling of these delicate soft tissues, which are often the primary source of pain and have a limited capacity for self-repair.
- Non-Pharmacological Pain Management: By reducing inflammation and directly impacting nerve-related pain signals, RLT offers a way to manage discomfort and improve the horse’s quality of life. This can be particularly useful for reducing reliance on long-term NSAIDs like Bute, thereby minimizing the risk of associated side effects.
The Prognosis: A Question of Variables
What’s the future? The one question every owner asks and the answer is… it varies. Wildly. The prognosis is fair to guarded and it depends on several factors:
- Severity and Type of Pathology: This is the biggest variable. A horse with mild osseous remodelling has a much better prognosis than one with a DDFT lesion. Soft tissue involvement is always a bigger concern.
- Chronicity: Early diagnosis and intervention correlates with better outcomes.
- Response to Initial Therapy: A positive response to therapeutic shoeing and initial medical management is a good sign.
- Owner Compliance and Dedication: Ultimately the owner is the case manager. Adherence to the farriery schedule, medication regime and exercise protocol is non-negotiable. Your commitment is a key determinant of success.
Final Points
A diagnosis of navicular syndrome is a big challenge. It tests an owner’s resolve. But you’re not helpless. While there’s no cure, a well managed comprehensive plan can make all the difference. It requires a partnership with your vet and farrier, understanding of the pathology and commitment to managing the whole horse. It’s a marathon not a sprint. But with proactive and compassionate care you can give your horse the best quality of life.
Common Questions
Check out the common questions below.
What’s my part in managing stress and rest to improve the prognosis?
You are the key; you are the horse’s daily manager. Your main job is to reduce biomechanical stress on the compromised structures. This means sticking to the vet-prescribed balance of controlled, low-impact exercise and rest. You must be the one to know when a planned activity is not suitable for the horse’s current comfort level. Any deviation from the management plan, improper exercise, delayed farriery, can exacerbate the pathology and create more problems. You are the chief executive of the treatment plan.
Why does the vet evaluate more than the bone if it’s called “navicular disease”?
Because the pathology is rarely confined to the bone. This is a common myth perpetuated by the name. The vet must assess the whole podotrochlear apparatu, the DDFT, the navicular bursa, the supporting ligaments and the vascular supply, to determine the true source(s) of pain. Calling it “navicular disease” is a misnomer; it’s a syndrome, a collection of interrelated pathologies. A treatment plan can’t be formulated without a full diagnosis of which components are affected.
How does palmar foot pain lead to secondary back pain?
Through a mechanism of compensatory gait alteration. A horse with heel pain will change its gait to minimize impact on that area, often landing toe-first. This abnormal biomechanical pattern disrupts the whole kinetic chain. To accommodate this altered gait the horse must recruit muscles in its back, pelvis and hindlimbs in an unnatural way. This sustained, abnormal loading pattern leads to muscle fatigue, myofascial strain and eventually chronic pain and potential articular changes in the back and hindquarters.
Once the severity of the damage is known, what else affects the prognosis?
The level of initial damage is a key indicator but not the only one. Other factors are massive. The horse’s intrinsic conformation is important, some hoof and limb structures are harder to manage. The strength of the horse’s digital circulation affects its healing ability. And most critically, owner management. A mild case can deteriorate quickly with poor management and a severe case can be managed surprisingly well for years with an exceptional owner. The long term outcome is a sum of all these.




